


A roadmap to improving our woeful rates of skin cancer
Saving money as well as lives ...
The Melanoma Network of New Zealand (MelNet), has just released its new Strategy for the Prevention and Early Detection of Skin Cancer in New Zealand.
Paraphrasing their CEO, Katrina Patterson:
Skin cancer is a huge public health issue in our country, impacting nearly 100,000 New Zealanders every year, and claiming 500 lives. Yet it is our most preventable cancer. The Strategy will not only serve as a roadmap for our prevention and early detection efforts but also provide a compelling case for urgent action and greater ongoing investment in this area. The evidence is compelling – consistent investment between now and 2050 could help prevent more than 400,000 skin cancers, save nearly 2,000 lives and avoid $700 million in treatment costs.
There are three main documents in the Report, which is accompanied by some useful resources including video clips and tool kits for various sectors of the population.
For me the most interesting parts were the many great graphs in the Supplementary Information section. This includes charts of cancer rates by time, gender, ethnicity, age group, and skin cancer type. They show that risk increases dramatically with age. The risk for seniors exceeds that for youths by more than a factor of 100. But don’t assume you’re bullet-proof just because you’re young. Any skin damage caused by overexposure in your youth may come back to bite you in your dotage.
The plots clearly demonstrate that while our incidence rates of melanoma are still increasing, there has been a slight drop-off in the most dangerous invasive form of the disease. One piece of good news is the rapid reduction in death rates from melanoma since the availability of immuno-therapy drugs like Keytruda, which was approved for use in New Zealand in September 2016 (more than two years after it was approved for use in the USA).

The mortality risk for men is nearly twice that for women. These higher rates for men may reflect different attitudes or different exposure patterns.
There are large ethnic differences, as shown for the number of cases per year of invasive melanoma in the plot below. According to the last census, the breakdown of New Zealand’s population by these four categories was 68 percent European, 18 percent Māori, 17 percent Asian, and 9 percent Pacific Islanders (Pacifica).

Case-numbers are hugely dominated by Europeans, although they represent only two thirds of the population. At the other extreme, the rapidly increasing Asian population - now rivalling Māori in number - hardly features on the graph. While the population of Māori is just twice that of Pacifica, there are at least 5 times as many cases. The number of cases per year, especially for Māori, has increased appreciably since the turn of the century. However, another plot from the report shows that the age-standardised rate for the population as a whole has remained has remained relatively constant, with a slight increase among older people being balanced by a decrease among younger people.
At the risk of annoying some, I think it must be said that the statistics for ‘Māori’ may be biased high for these statistics that depend on skin type because in many cases, after two centuries of colonisation, the bloodline (and skin type) can be predominantly European. The rapid increase in invasive melanoma in the last two decades may simply be a reflection of the greater intermixing in those who identify as ‘Māori’ (there’s little choice for nuances when filling out the NZ census form). The relatively lower (but increasing) rates for Pacifica, most of whom have a similar ethnic background to Māori, may be due to their more recent migration from their more isolated country of origin to New Zealand. I suspect that Māori with similar skin colouring will have similarly lower rates.
The incidence rates for skin cancer among Māori are typically only 2 percent of those from non-Māori, but for those who identified as Māori in 2021 (of whom most will have some European blood), the incidence of invasive melanoma is around 7 percent of that for non-Māori. The poorer prognosis for Māori is possibly due to later diagnosis, or lack of access to medical treatment.
The report also touches on matters closer to my heart, by showing where in the country the risk from over-exposure to UV radiation is greatest. It’s based on data that my colleague, Ben Liley, contributed to generate new maps like the one below where the UV risk is broken down by administrative region.
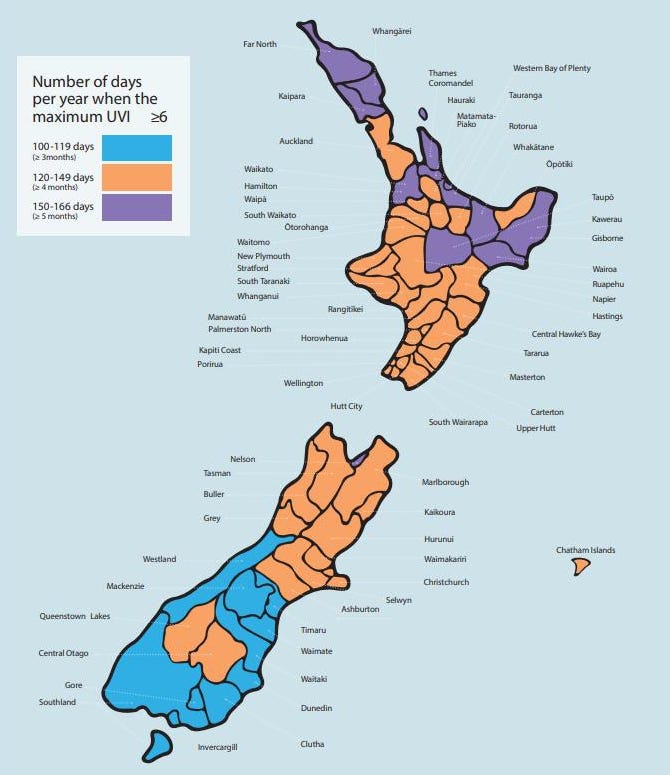
The peak UVI that occurs in New Zealand can exceed 12. That value of 6 is the threshold for UV being designated as ‘High’, with skin damage for some occurring with less than 30 minutes of exposure. As you can see, throughout the country there are at least 100 days per year when the UVI exceeds 6, rising to more than 150 days per year in some regions. The risk generally increases from south to north, but there are regional differences due to different cloud amounts and sunshine hours. Where I live in sunny Central Otago, the risk (by this measure) is greater than over the rest of the lower South Island, but still less than in Northland and sunnier regions in the upper half of the North Island.
Check out the other figures here.
Thanks Richard. Do you see personal wearables helping?
Hi Richard, I find your topics incredibly relevant for Tasmania where I live. I'm the State Manager of Melanoma Institute here. Tasmania's incidence of melanoma is second behind Queensland and I suspect the reasons mirror those of NZ (including lack of respect of UV and apathy around use of personal protection) Thanks for your work